Table of contents
Do you want more traffic?
Hey, I'm from FTA Global. I'm determined to grow a business. My only question is, will it be yours?


The first thing we did wasn't launch anything. It was to instrument everything.
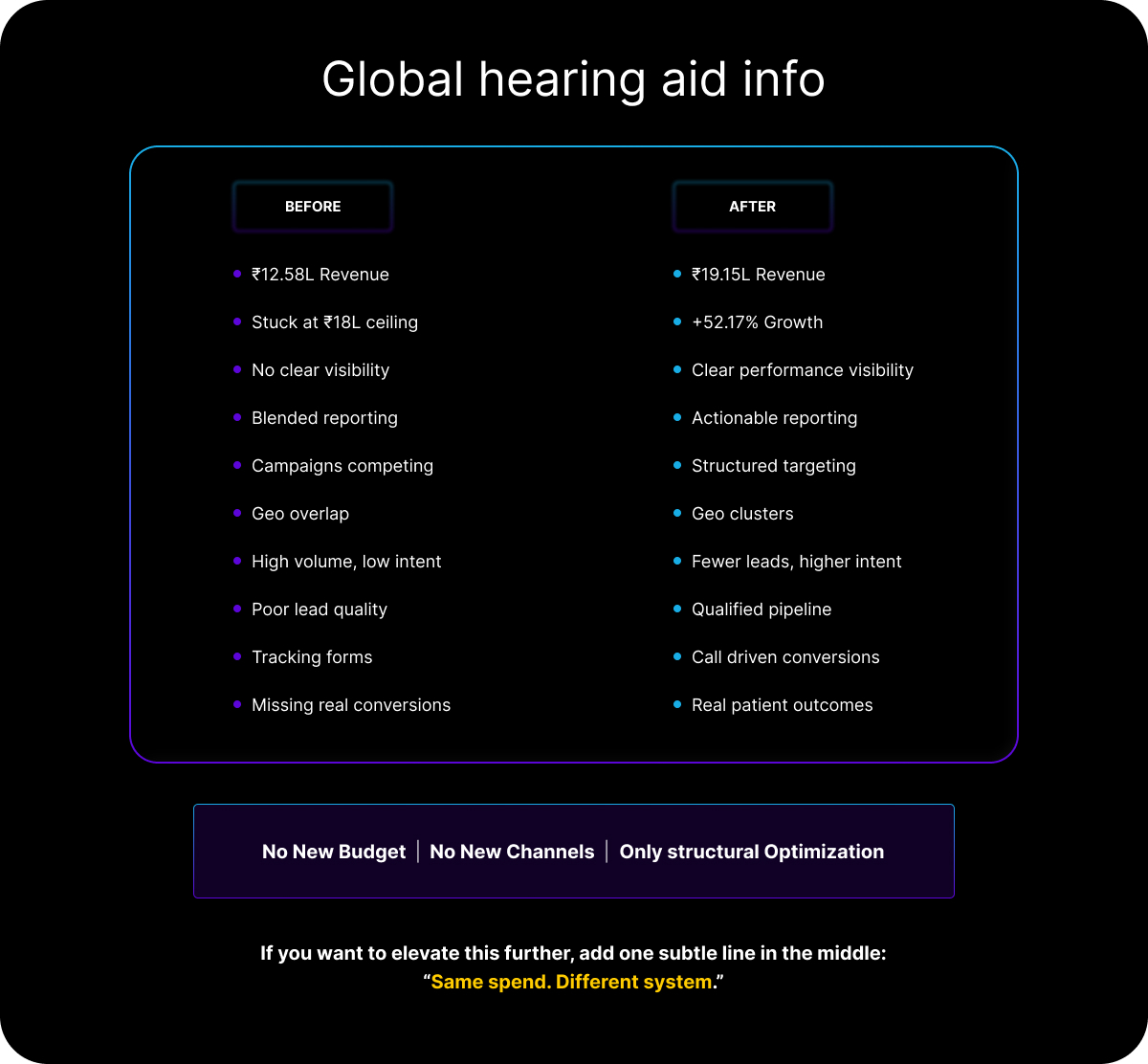
There was no clean channel-level or campaign-level reporting in place. Decisions were being made on blended metrics the kind that make everything look acceptable and nothing look fixable. You can't optimize what you can't isolate.
Once we had proper visibility, four structural problems became immediately obvious.
The geo targeting was eating itself. Campaigns across clinic locations were overlapping significantly. Multiple ads were targeting the same users in the same areas, bidding against each other in the same auction. The brand was competing with itself and paying for it.
High-potential regions weren't being activated. There were markets with genuine demand signals and zero meaningful campaign presence. Not underperforming just absent.
The campaigns were optimizing for the wrong conversion. Form fills were being treated as the primary success metric. But in healthcare especially audiology the real conversion is the inbound call.
A patient ready to book an appointment picks up the phone. They don't fill out a contact form and wait.
Lead quality had no floor. Volume was coming in, but there was no qualification layer. The sales team was spending time on leads that were never going to convert, which meant the actual cost of a real patient was far higher than the CPL metric suggested.
We rebuilt the geo targeting from scratch. Instead of targeting by individual location, we restructured into smart geographic clusters grouped by proximity, audience density, and clinic catchment areas. This eliminated bid cannibalization and made budget allocation logical instead of accidental.
We launched call-first campaigns. Dedicated campaigns built entirely around inbound call conversion, not form fills. Ad copy, landing pages, and bidding strategies all oriented toward getting the phone to ring from someone who actually intends to come in.
We went vernacular in underactivated markets. Regional audiences don't convert on generic national creative. We rebuilt ad copy, creatives, and lead forms in local languages for specific high-potential geographies. Relevance drives trust. Trust drives calls.
We added a qualification layer. OTP verification and intent-based filters at the lead stage. The goal was simple: ensure that the volume we were generating reflected real, reachable patients not just form submissions.
We built dashboards that actually told us something. Channel-level, campaign-level, geography-level reporting so every optimization decision had a clear evidence base.
October: ₹12.58L. Baseline established. Structural fixes begin.
November and December: Campaigns restructured, clusters deployed, call-focused creatives live, vernacular ads running. The system starts responding.
December milestone: ₹18.36L. First time in the brand's history that monthly revenue entered the ₹18–20L target range.
January: ₹19.15L. All-time record. 52.17% above where we started.
Simultaneously, Cost Per Lead dropped 8.07%. This matters more than most people acknowledge. Revenue going up while CPL going down meaning we were not just spending to a bigger number but generating more efficient growth.
